Gallery Before & After


OtoplastyGIFs
See All Otoplasty GIFs



Actual Patient

Ear reshaping requires a surgeon who not only specializes in facial anatomy but has a keen eye for facial aesthetics. Approximately 5% of the population has overly prominent ears. Otoplasty is the name of the procedure where a part or parts of the ear are reshaped so that the ear looks less prominent.
Otoplasty surgery in Chicago with Dr. Shah is typically a relatively pain-free experience. He has pioneered a technique that allows him to perform ear surgery as an in-office procedure. In addition, he has co-authored an article on Otoplasty which describes generalities about the procedure.


Nisi adipisicing enim amet veniam sunt ut qui voluptate sunt fugiat proident officia. Dolore officia exercitation et sunt aute fugiat amet id magna duis laborum in. Dolore irure tempor do ea excepteur. Quis fugiat cupidatat proident exercitation. Ullamco consequat dolor qui sunt voluptate sint Lorem commodo proident aliqua dolor incididunt nisi incididunt ea. Pariatur est elit velit.


The external ears are made of cartilage and skin. There is a robust blood supply and nerve supply to the ear, making the ears sensitive to touch as well as highly vascular.
Like other parts of the body, the ear has specific terminology to describe specific components of the external ear. On the periphery of the ear there is the helix, tragus and lobule. Within the ear, there lies the conchal bowl and antihelical fold.
There are several techniques for otoplasty (ear reshaping) that are used to help reshape the ear. Each technique is used for a different aspect in ear reshaping. For patients seeking ear surgery in Chicago, Dr. Shah utilizes advanced otoplasty methods tailored to each individual’s anatomy and goals.
The Mustarde suture is one of the most powerful techniques used in otoplasty. It is used when the antihelical fold is under developed, which causes the top portion of the ear to stick out further.
The prominent helix is typically caused by a failure of the antihelical fold to form. This can cause the ear to stick out further from the mastoid (back of ear) then desired. Far and away, the most common technique to correct this is the Mustarde suture. This is where the surgeon attempts to recreate the antihelical fold by placing sutures parallel to the helical rim. By placing a series of sutures here the antihelical fold can be created. Dr. Shah only recommends the use of permanent sutures which are braided. Non permanent sutures are not as effective in long term maintenance of the ear and can lead to earlier relapses. Non braided sutures have too much memory and can create unintended cuts through the delicate cartilage of the ear.

The conchal bowl is the portion of the ear that can make the cup of the ear look too prominent. This can be from a combination of factors which includes excessive cartilage formation, poor angulation between the ear and the head.
Correction of the prominent conchal bowl may be done with a suture using what is called a setback sutures.

Earlobes can become stretched with age, loss of elasticity, or the use of heavy earrings over time. Correction of prominent ears is typically an in office procedure with local anesthesia. The excessive length of the earlobes is reshaped by exact excision of the prominent portion. Most patients can wear earrings 4 to 6 weeks after the procedure. We don’t recommend the use of heavy earrings.


Otoplasty will not change hearing in either a positive or negative manner. The mechanism for hearing takes place in the middle and inner ear.
Otoplasty costs depend on several factors including the type of reshaping, the type of anesthesia, and the anticipated length of time surgery will take. In general, otoplasty with light sedation will cost significantly less than otoplasty requiring general anesthesia. As with any plastic surgery procedure, price should not be the reason for picking a surgeon.
Pixie ear repair can range from a simple office procedure to a need for a redo facelift. Most pixie ears are a result of excessive tension placed on the earlobes, causing them to stretch inferiorly after a facelift settles. An experienced surgeon can advise the best course of action to fix a Pixie ear in the least invasive and most effective manner.
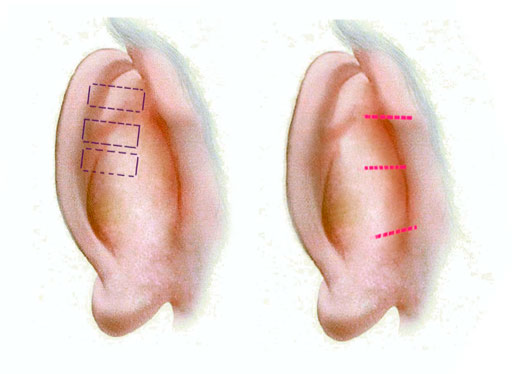
One of the biggest challenges of otoplasty is creating symmetry post procedure. Dr. Shah performs precise caliper measurements of the superior, middle, and inferior portion of the ear both pre procedure and post procedure allow the surgeon an objective means of adjusting the degree of “pinning” the ears back. Dr. Shah will create symmetry by using measures as well as understanding the healing course that takes place during otoplasty.
This is perhaps one of the bigger concerns after an otoplasty. Many patients wear hair in a manner to conceal the size of their ears, and post procedure plan on having their ears on full display. A poorly executed scar can take away any benefit from an otoplasty. Dr. Shah uses precise and meticulous closure with close follow up which leads to scars which are difficult to see.
Earlobe reduction requests have become increasingly popular over the last several years. An elongated earlobe can signify aging. Ear lobes can be reduced in the office comfortably under local anesthesia.
Typically, most insurance companies do not cover changes that are due to appearance with the exception of traumatic repair which is medically necessary. Torn ear lobes do not fall into that category. Ear lobe piercing repair for slightly larger ear piercing may or may not require repair. Factors which must be accounted for are:
Unfortunately, poor scarring after an otoplasty is not an unusual thing to see in with many surgeons. This can be a big factor in your ability to wear hair short or pulled back in a ponytail. Dr. Shah closes your scar meticulously and without tension to minimize the occurrence of this. Some steps such as kenalog injections or silicone sheeting can be helpful in select cases as well.
There are various phases during the recovery process of a well executed otoplasty performed by a surgeon with expertise in ear reshaping:
Ears stop growing at around the age of 5 or 6. Ears will lose elasticity over time making them appear longer. However, these changes occur over a long period of time. The changes that occur after an otoplasty are permanent.
Nearly 5% of the population has prominent ears. Most causes of prominent ears are inherited.
A cup ear is where the concha of the ear is overdeveloped causing the ear to cup out.
A lop ear is where the top of the ear lacks an antihelical fold, causing the top portion of the ear to be more prominent.
Cartilage splitting techniques refers to techniques which excise cartilage. Cartilage sparing techniques refer to those techniques which spare the cartilage, most typically using sutures to reshape the ear. Dr. Shah uses a tailored approach to reshaping the ear to provide a natural contour change to the ear. He bases his technique on the individual anatomy of the patient.
Otoplasty is an individual choice as is plastic surgery.
There are few medical contraindications to an otoplasty. Patients with a history of chondritis and chronic draining ear infections are not ideal candidates. Patients with a history of keloid or hypertrophic scars should be aware that there is a possibility for keloid formation post procedure and need for kenalog injections.
The ear hears through sound passing through the external auditory canal, hitting the tympanic membrane and ossicles and finally reaching the cochlea before traveling to the brain. Any impedance along the way can affect hearing. It is extremely uncommon for an otoplasty to affect hearing. In patients with setback sutures, if the surgeon places the suture too close to the external auditory canal, a narrowing of the canal can occur, which could potentially affect hearing.
A Darwinian tubercle is a portion of the ear thickened near the superior and middle pole of the ear. see picture (get sam shah ear). Darwinian tubercles are common variants of a normal ear seen in approximately 10% of the population. In some patients, the size, shape, or asymmetric nature of a Darwinian tubercle can be a source of frustration. Decreasing the tubercle can be accomplished at the same time as an otoplasty by shaving down the helix. In cases of isolated Darwinian tubercle issues or with large tubercles, an anterior approach can be utilized.
The lower portion of the ear is addressed by finding the root cause of the prominence. In patients with prominent ear lobes, an earlobe reduction or pexy can be performed. If there is excess cartilage in the area, the lower part of the helical cartilage (caudal aspect) can conservatively trimmed as can the conchal bowl.
This is where the surgeon aggressively sets back the middle of the ear in relation to the upper and lower portion of the ears. This creates the appearance of a telephone. Dr. Shah fixes patients with poor otoplasty outcomes by defining what is the main issue with the ear. Most commonly, failure to adequately correct the superior and lower pole has created a telephone deformity to balance the appearance of the ear.
In this case, the superior and lower poles are too close to the head in relation to the middle portion. This may result in either releasing setback sutures or reducing the size and shape of the conchal bowl.
There are two factors which can make an ear look prominent. First of all, there is ear projection or how far the ear sticks out from the head. The further the ear sticks out from the head, the more attention it will draw to itself. The other factor which makes ears look prominent is the relative size of the ears to the other facial structures and the head. Size is typically measured from the top of the ear to the ear lobe. In otoplasty, projection and size are addressed by a variety of ear maneuvers to bring the ear closer to the head and actually decrease the surface of the ear depending on the case.
No, even in long haired patients the incision is made behind the ear in the post auricular crease.
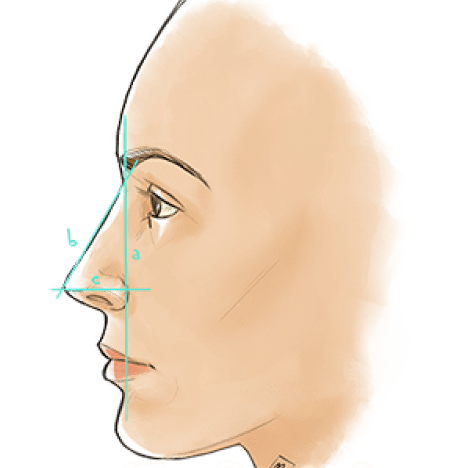
The ear is typically measured in three locations, the top of the ear, the middle, and the bottom of the ear in relationship to the bony portion behind the ear called the mastoid. Normally, the ear protrudes about 11 mm from the top of the ear, 17 mm from the middle third, and 21 mm along the lower portion. The concha (or bowl of the ear) is typically 14 mm from the mastoid of the ear. Another way to analyze the ears is to measure the helix and the mastoid should be about 20 degrees. In patients with prominent ears, the ears will protrude at least 30 degrees.
The length of the ears are typically 6 cm while the width of the ear is around 3.5 cm
Dr. Shah only recommends the use of permanent sutures which are braided. Non permanent sutures are not as effective in the long term maintenance of the ear and can lead to earlier relapses. Non braided sutures have too much memory and can create unintended cuts through the delicate cartilage of the ear.
Scoring of the ear is done on a case by case basis depending on an individual’s anatomy.
Any permanent suture may be rejected by the body or extrude.
Most patients can wear earrings 4 to 6 weeks after the procedure. We don’t recommend the use of heavy earrings.
Scars in the earlobe conceal well.
Typically about a week. It is best done under a break during the school year. Activity can be slowly increased as the child’s recovery progresses.
If you live near Chicago, IL, Anil Shah Facial Plastic Surgery offers otoplasty among its services and is conveniently located at 200 West Superior St., Suite 200 Chicago, IL 60654