


Zygomaticus Major Muscle Landmark
A Practical Landmark in Identifying the Zygomaticus Major Muscle
Objective:
Analyze the efficacy of the newly described “zygomaticus notch” in identifying the zygomaticus major in both a freshly preserved cadaver study and in clinical applications.
Study Design:
Cadaver dissection and clinical study
Methods:
23 fresh cadaver facial halves were dissected. Four reference points were identified in each cadaver head: the zygomatic arch, the malar eminence, the modiolus, and the zygomaticus major insertion notch which is a palpable landmark identified midway between the Zygomatic arch and malar eminence. A straight line was drawn from the zygomaticus major insertion notch to the modiolus. An additional line was drawn from the malar eminence to the modiolus. An incision was made along the each line to the depth of the facial muscles. The presence or absence of zygomaticus major muscle was recorded. Clinically, the zygomaticus insertion notch was palpated in 58 patients who received deep plane rhytidectomy over a span of two years.
Results:
The zygomaticus major insertion notch was palpated and identified in 23/23 facial halves. The zygomaticus major insertion notch was accurate in identifying the course of the zygomaticus major muscle in 23/23 facial halves. The line created by the malar eminence to the modiolus was inaccurate in 23/23 facial halves. Clinical application revealed proper identification of the zygomaticus major in 58/58 patients.
Conclusion:
The zygomaticus major insertion notch is a reliable landmark for the identification of the zygomaticus major muscle.
INTRODUCTION
The identification of the course of the zygomaticus major muscle plays an important role in facial plastic surgery. First of all, it serves as an important landmark in deep plane rhytidectomy. (1) Since the facial nerve courses deep to the plane of the zygomaticus major, providing the facelift surgeon a reliable guide to dissection into the medial portion of the face. (1,2) Additionally, some surgeons report plication of the zygomaticus muscle to provide rejuvenation of the aged face. (3,4) For patients receiving BOTOX injections periorbital, the location of the zygomaticus major muscle is critical to prevent the unwanted sequelae of a lip drop. (5)
The zygomatic muscle is responsible for lifting the corners of the mouth, used primarily in smiling. It is typically a fan-shaped muscle, which may be single-headed or bifid in nature. The muscle increases in size and thickness in males and in patients with increasing BMIs.
Located anterior to the zygomaticus major muscle is the zygomatic cutaneous ligament, aka Mac Gregor’s patch. The release of this ligament is crucial in providing mobilization of the malar fat pad and rejuvenation of the midface structures. The SMAS layer can be mobilized further and with less tension with the release of this ligament. A back cut of the zygomaticus major muscle itself will also provide improved mobilization of the SMAS layer.
Deep to the zygomaticus major muscle lies the plexus of the zygomatic branch of the facial nerve. The orbicularis oculi may be partially innervated in some patients by some nerve branches which lie superficial to the zygomaticus major muscle, but due to the plexiform innervation and vast majority of nerves which lie deep to the zygomaticus major muscle, lending permanent sequelae are unlikely.
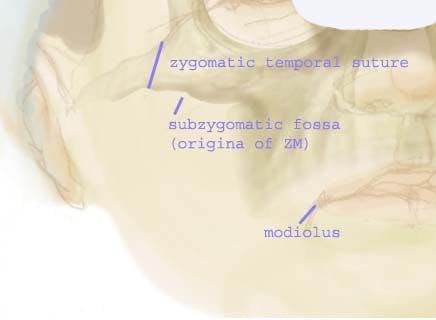
The zygomaticus major, along with the other upper lip mimetic muscles, insert at the modiolus. The zygomatic muscle originates anterior to the zygomatic temporal suture within the sub-zygomatic fossa. (6) (See diagram one)
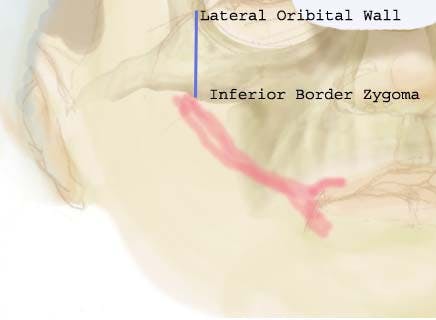
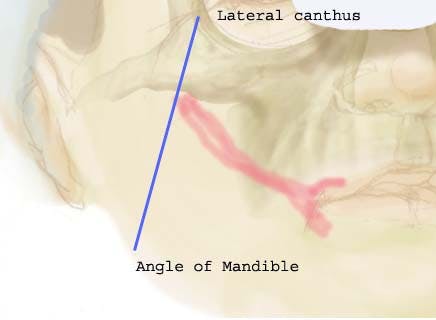
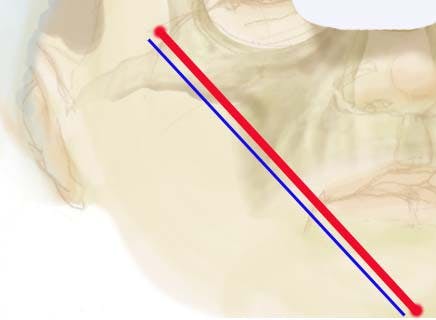
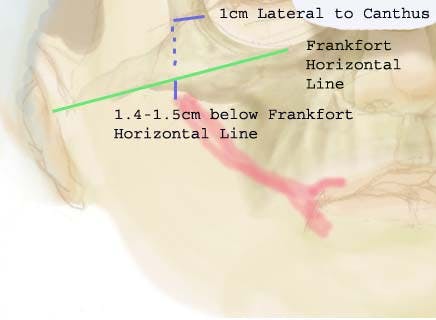
Despite this anatomic description, surgeons have sought complex means of ascertaining the clinical origin of the zygomatic major muscle. Mendelson described the origin by ” a vertical line dropped from the lateral orbital rim to the lower border of the zygoma.” Tramolada described t;he origin from the malar bone on a line drawn from the lateral canthus to the mandible. Furnas described the location to be along the zygomatic body coursing to the modiolus. In a more recent paper, Mowlavi and Wilhelmi found that the lateral border of the zygomaticus major was 4.4 mm lateral and parallel to an oblique line drawn from the mental protuberance to the notch defined as the most anterior-inferior aspect of the temporal fossa at the junction of the frontal process and temporal process of the zygoma.i Finally, Spiegel and DeRosa published an anatomical paper in which they describe the origin of the zygomaticus major at 1.40 cm inferior to the Frankfort horizontal line at 1 cm lateral to the lateral canthus.
While the previously described descriptions were fairly accurate in describing the course of the zygomaticus major muscle, their overall complexity has prevented them from being universally adopted by facial plastic surgeons. The origin of the zygomatic muscle is the subzygomatic fossa, which is located posterior and inferior to the malar eminence and anterior to the zygomatic temporal suture. Despite some contrary reports, the zygomatic fossa is an easily palpable landmark. The senior author has developed a technique for locating the course of the zygomatic muscle. By utilizing the palpable subzygomatic fossa itself, the location of the zygomatic muscle can be ascertained.
METHODS
Twenty-three fresh cadaver facial halves were dissected. Four reference points were identified in each cadaver head: the Zygomatic arch, the malar eminence, the modiolus, and the subzygomatic fossa which is a palpable landmark identified midway between the zygomatic temporal suture and malar eminence. A straight line was drawn from the zygomaticus major insertion notch to the modiolus. (Figure 1 and 2) An additional line was drawn from the malar eminence to the modiolus. An incision was made along the each line to the depth of the facial muscles. The presence or absence of zygomaticus major muscle was recorded when utilizing each of the above landmarks. The palpation of the landmarks was performed by a junior resident (SS) in order to ensure the ease of learning this technique.
The clinical application of the efficacy of the zygomaticus notch was applied in 58 consecutive deep plane rhytidectomy patients. The zygomaticus notch was identified and marked prior to the facelift, as well as the modiolus and proposed location of the zygomaticus major muscle. A deep plane rhytidectomy was performed with location of the zygomaticus major muscle using the external landmark as a guide.
RESULTS
The subzygomatic fossa was palpated and identified in 23/23 facial halves. The zygomaticus major insertion notch was accurate in identifying the course of the zygomaticus major muscle in 23/23 facial halves. The line created by the malar eminence to the modiolus was inaccurate in 23/23 facial halves.
Clinically, the location of the subzygomatic fossa correlated well with 58 consecutive patients and the location of the zygomatic major muscle located.
DISCUSSION
The authors of this paper found the subzygomatic fossa (PJM, SS, AS) an easily palpable landmark. As the origin of the zygomatic major muscle, it make more clinical sense to use this as a landmark, rather than a complex and tedious correlation. We found both the palpability of the subzygomatic fossa and its underlying relationship with the origin of the zygomatic major muscle to be highly accurate.
Landmarks are useful in surgery to provide the surgeon an appropriate reference to the surrounding structures. In order for a landmark to be useful, it must be accurate and identifiable.
The use of the zygomaticus major muscle was a landmark in deep plane rhytidectomy is limited by tedious previous descriptions on the origin of this muscle. The subzygomatic fossa simplifies its location and can allows for the identification to readily occur.
Minimizing complications in procedures such as BOTOX are crucial to providing optimal patient results. Zygomaticus major muscle paralysis has been reported as an inadvertent target with periorbital rhytids. Limiting the dilution content of BOTOX, experience with injection, and knowledge of the facial anatomy all will limit this potential sequlae. A simple technique to palpate the subzygomatic fossa lets the surgone
The deep plane facelift require extensive knowledge of anatomy in order to perform it safely. The zygomaticus major is one important landmark in performing the deep plane facelift safely and effectively. With incorporation of this landmark it is hoped that the identification of this muscle will provide improved safety in deep plane rhytidectomy.
