


Saddle Nose Deformity
Saddle Nose Deformity is a condition where the support of the nose is weakened whereby the nose is “saddled” in the middle. This deformity has also been called a boxer’s nose deformity or pug nose. The underlying cause is typically less of septal support. This can be caused by a variety of conditions which includes facial trauma (punch to nose, septal hematoma), overaggressive septoplasty or rhinoplasty, or use of cocaine.
Trauma creates a saddle nose by either directly fracturing the septal cartilage and/or bone or by creating a condition known as a septal hematoma. A hematoma is a collection of blood. This collection of blood prevents nourishment from reaching the septal cartilage and can create a hole in the septal cartilage. The weakening of the septum can lead to collapse of the nose.
Cocaine acts to vasoconstrict, or tighten the blood supply, to the nose. By turning off the nourishment to the nose, the septal cartilage can again collapse.
Overaggressive rhinoplasty can lead to loss of septal support. Surgeons performing rhinoplasty must be comfortable with advanced septoplasty maneuvers, as the septum is the foundation of a properly executed rhinoplasty and functional airway.
The treatment of the saddle nose deformity is to reconstruct the septal cartilage and/or bridge of the nose to provide improved appearance and function. Some patients with saddle nose deformity will have an associated septal perforation which may or may be able to be addressed depending on its size, location and orientation. Often times patients will require either costal cartilage grafting or auricular cartilage grafting to improve contour of the nose.

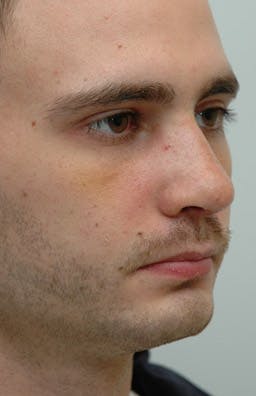




Figure Legend. Patient from England (London area) who noted collapse of his nose after years of boxing. His biggest complaint was that his nose looked too effeminate and that he had difficulty breathing through it. He did not want to use costal cartilage, so auricular cartilage was used as an alternative.
His postoperative views (2 weeks postoperative) demonstrate improvement of his bridge and nasal tip. This case also illustrates that when the nose is expanded, the nose made larger and the dorsum higher, often times the appearance of the nose and swelling is not as dramatic as when the nose is reduced in size through an open approach.
