


Cartilage Grafting from the Ear to the Nose
Auricular cartilage grafting and rhinoplasty and nasal reconstruction
What is auricular cartilage grafting?
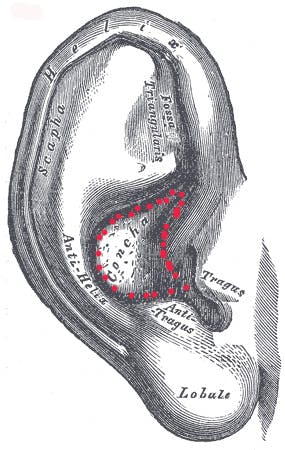
Auricular cartilage grafting is taking cartilage from the ear to reconstruct the nose. Typically grafts are taken from the concha cymba and cavum of the ear (MARKED IN RED) to remove cartilage without changing the overall shape of the ear. The skin of the ear is intact.
What are the techniques to remove cartilage from me ear?
An anterior or posterior approach are the two most common methods. In the anterior approach, the surgeon will make scar on the front surface of the ear. In the posterior approach, the surgeon will make the scar on the posterior surface of the ear.
Dr. Shah prefers the posterior approach because the scar is better concealed. In addition, Dr. Shah feels it is a more predicatable method to remove auricular perichondrium. Auricular perichondrium is the “carpet of the ear”. This carpet can be used to soften the use of grafts and make them much less visible.
Why is perichondrium so important?
Perichondrium offers the surgeon a permanent solution to graft and tip camouflage. In thin skinned patients, the risk of shink wrapping is a very real phenomenon. By placing a natural barrier between the skin and the cartilage, this phenomenon can be reduced in appropriate patients. The thickest perichondrium is costal cartilage perichondrium. Auricular perichondrium is less thick.
In the past, surgeons have used Alloderm to act as a buffer layer between skin and cartilage. However, Alloderm has several disadvantages. First of all, it is derived from cadaver skin (human). Additionally, Alloderm does not last permanently. It will act as a barrier early on, but will eventually dissolve, prolonging the shrink wrap phenomenon, but not preventing it.
Do you use Alloderm?
I use Alloderm in two specific circumstances. First of all, in septal perforation repair ( a hole in the nasal septum), it acts as a barrier from both flaps adhesing. In dorsal augmentation, Alloderm (thick sheet) or even Permacol can act as a scaffolding for dorsal augmentation. My preference for dorsal augmentation is single pieces, carved and camouflaged with perichondrium. Sometimes multiple pieces of cartilage are sutured together. In order for the cartilage pieces to lay flat and attempt to recreate the feel of a single piece, I use Alloderm to act as PLATFORM.
Do you ever make an incision anteriorly along the ear?
Yes, when harveting composite cartilage grafts. Composite cartilage grafts are a composite of two different tissues, cartilage and skin. These grafts are used for a variety of purposes in nasal reconstruction and rhinoplasty including, alar retraction, short nose patients, overly narrow nostrils, soft tissue triangle absence, etc. They are valuable grafts in the revision rhinoplasty surgeon’s aresenal.
Since skin is removed, the concha cymba is the preferred location for harvesting the conchal cartilage graft for several reasons. Its location facilitates easy closure, minimizes external ear changes, and the skin is tightly adhered in this location.
So will my ear look the same after auricular cartilage grafting?
After typical auricular cartilage harvest, the ear will look the same. Early on during the healing process, the ear will stick slightly out from the head (proptotic) but will return once the swelling dissipates. Your ear will feel slightly softer than prior to surgery in the location of harvest. However, surprisingly, even then it is pretty difficult to determine, even by most plastic surgeons, that you have had ear cartilage removed.
I don’t want auricular cartilage grafting. I just want a rhinoplasty.
Unfortunately, some more complex cases benefit tremendously from cartilage grafting. Some cases need cartilage grafting to support the nose properly, augment the nasal bridge, support external and internal valves, etc.
What are the disadvantages of auricular cartilage grafting?
Auricular cartilage grafting has several disadvantages due to its soft, curved nature. First of all, asymmetries are much more visible. Auricular cartilage is not the first choice for dorsal augmentation. For severe alar collapse, auricular cartilage does not offer significant enough support. My preference for auricular cartilage is in reconstruction of the middle vault, radix grafts, alar rim grafts, tip contouring grafts, and columellar filler grafts.
Due to its lack of significant strength, I do not like to use auricular cartilage for total septal reconstruction, septal extension grafts. Due to the prominent curves associated with it, I do not like to use it for lateral crural repositioning. I have used auricular cartilage grafting in the past for all of these reasons with satisfactory results. However, I think better grafting options are available to the surgeon.
My first preference for cartilage grafting is septal. Depending on the needs of the patients, costal cartilage or auricular cartilage may be my next preference.
Auricular cartilage is typically harvested from a posterior auricular approach meaning the incision is behind the ear in the crease of the ear. The incision here allows access to the concha cymba and concha cavum. Cartilage can be removed while maintaining the integrity of the skin anteriorly along the front of the ear. The ear typically will look the same, however will feel slight softer where the cartilage has been removed. Ear cartilage harvest is typically somewhat uncomfortable for the patient since the ear is highly sensitive and innervated structure on the face. Auricular cartilage harvest does not affect hearing.
“The nose should fit the face”
A strong jawline would suggest a stronger nose.
